Factors Behind Hammer Toes
 Overview
Overview
Hammer toes and mallet toe are two foot deformities that occur most often in women who wear high heels or shoes with a narrow toe box. These types of footwear may force your toes against the front of the shoe, causing an unnatural bending. A hammertoe has an abnormal bend in the middle joint of a toe. Mallet toe affects the joint nearest the toenail. Hammertoe and mallet toe are most likely to occur in the toe next to your big toe. Relieving the pain and pressure of hammertoe and mallet toe may involve changing your footwear and wearing shoe inserts. If you have a more severe case of hammertoe or mallet toe, you may need surgery to experience relief.
Causes
Medical problems, such as stroke or diabetes that affect the nerves, may also lead to hammertoe. For example, diabetes can result in poor circulation, especially in the feet. As a result, the person may not feel that their toes are bent into unnatural positions. The likelihood of developing hammertoe increases with age and may be affected by gender (more common in women) and toe length; for example, when the second toe is longer than the big toe, hammertoe is more likely to occur. Hammertoe may also be present at birth. Genetics may factor in to developing hammertoe, particularly if the foot is flat or has a high arch, resulting in instability.
 Symptoms
Symptoms
Hammer toes can cause problems with walking and lead to other foot problems, such as blisters, calluses, and sores. Pain is caused by constant friction over the top of the toe?s main joint. It may be difficult to fit into some shoe gear due to the extra space required for the deformed toe. In many cases there will be pain on the ball of the foot over the metatarsals along with callus formation. This is due to the toes not functioning properly, failing to properly touch the ground during the gait cycle. The ball of the foot then takes the brunt of the ground forces, which causes chronic pain.
Diagnosis
Your healthcare provider will examine your foot, checking for redness, swelling, corns, and calluses. Your provider will also measure the flexibility of your toes and test how much feeling you have in your toes. You may have blood tests to check for arthritis, diabetes, and infection.
Non Surgical Treatment
Symptomatic treatment of hammertoes consists of such things as open toed shoes or hammertoe pads. There are over the counter corn removers for temporally reducing the painful callous often seen with the hammertoe. These medications must be used with caution. They are a mild acid that burns the callous off. These medications should never be used for corns or callouses between the toes. Persons with diabetes or bad circulation should never use these products.
Surgical Treatment
In advanced cases in which the toe has become stiff and permanently bent, the toe can be straightened with surgery. One type of surgery involves removing a small section of the toe bone to allow the toe to lie flat. Surgery for hammertoe usually is classified as a cosmetic procedure. Cosmetic foot surgeries sometimes result in complications such as pain or numbness, so it's better to treat the problem with a shoe that fits properly.
 Prevention
Prevention
Walking barefoot increases the risk for injury and infection. Being on your feet throughout the day can cause them to swell, this is the best time to buy shoes to get a better fit. Do not buy shoes that feel tight. Do not buy shoes that ride up and down your heel as you walk. The ball of your foot should fit into the widest part of the shoe. Remember, the higher the heel the less safe the shoe will be. Avoid shoes with pointed or narrow toes. If the shoes hurt, do not wear them. If you start noticing the beginning signs of hammer toes, you may still be able to prevent the tendons from tightening by soaking your feet every day in warm water, wearing toe friendly shoes, and performing foot exercises such as stretching your toes and ankles. A simple exercise such as placing a small towel on the floor and then picking it up using only your toes can help Hammer toe to restore the flexibility of tendons.
What Is Overpronation Of The Feet
Overview
Pronation is the inward movement of the foot as it rolls to distribute the force of impact of the ground as you run. The foot "rolls" inward about fifteen percent, comes in complete contact with the ground, and can support your body weight without any problem. Pronation is critical to proper shock absorption, and it helps you push off evenly from the front of the foot. Although pronation is a natural movement of the foot, the size of the arch can affect its ability to roll, causing either supination (underpronation) or overpronation. If you have a normal arch, you're likely a normal pronator, meaning you'll do best in a shoe that offers moderate pronation control. People with flat feet normally overpronate, so they do well in a motion-control shoe that controls pronation. High-arched people typically underpronate, so they do best in a neutral-cushioned shoe that encourages a more natural foot motion.
Causes
During our development, the muscles, ligaments, and other soft tissue structures that hold our bones together at the joints become looser than normal. When the bones are not held tightly in place, the joints are not aligned properly, and the foot gradually turns outward at the ankle, causing the inner ankle bone to appear more prominent. The foot moves in this direction because it is the path of least resistance. It is more difficult for the foot to move in the opposite direction (this is called supination). As we develop, the muscles and ligaments accommodate to this abnormal alignment. By the time growth is complete, the pronated foot is: abnormally flexible, flat, and its outer border appears raised so that as you step down you do not come down equally across the entire foot; instead, you come down mostly on the inner border of the foot. Normal aging will produce further laxity of our muscles that causes the pronation to become gradually worse.
Symptoms
Over-pronation is a condition where the arch flattens out which makes the feet roll inward while walking. This condition is also known as flat feet. It imposes extreme additional stresses on the plantar fascia, a fibrous band of tissue which connects the heel to the forefoot. Over-pronation makes walking a painful experience because of the additional strain on the calves, heel and/or back. Treatment for over-pronation involves the use of specially-made orthotics which offers arch support and medial rear foot posting as corrective measures.
Diagnosis
The best way to discover whether you have a normal gait, or if you overpronate, is to visit a specialty run shop, an exercise physiologist, a podiatrist or a physical therapist who specializes in working with athletes. A professional can analyze your gait, by watching you either walk or run, preferably on a treadmill. Some facilities can videotape your gait, then analyze the movement of your feet in slow-motion. Another (and less costly) way is to look at the bottom of an older pair of run shoes. Check the wear pattern. A person with a normal gait will generally see wear evenly across the heel and front of the shoe. A person who overpronates will likely see more wear on the OUTside of the heel and more wear on the INside of the forefoot (at the ball). A person who supinates will see wear all along the outer edges of the shoe. You can also learn about your gait by looking at your arches. Look at the shape your wet feet leave on a piece of paper or a flat walking surface.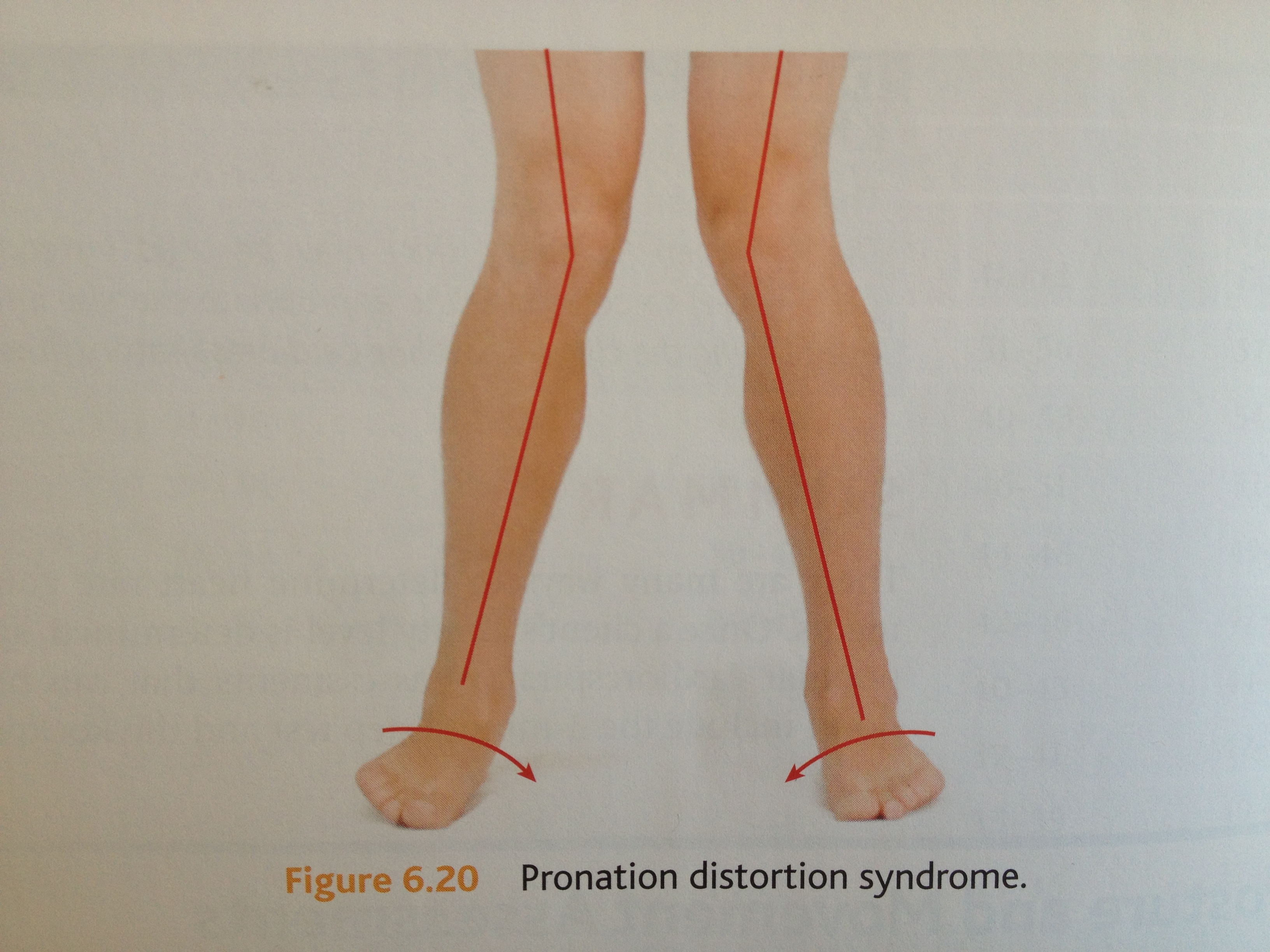
Non Surgical Treatment
Overpronation is usually corrected with orthotics and/or strengthening exercises for the tibialis posterior. Massage treatment can relieve myofascial trigger points in the tibialis posterior, and other muscles, and address any resulting neuromuscular dysfunction in the leg or foot. Biomechanical correction of overpronation might require orthotics, neuromuscular reeducation, or gait retraining methods, as well. Stretching the gastrocnemius and soleus muscles will reduce hypertonicity in these muscles and also is essential for effective treatment. Because of impacts throughout the remainder of the body, the detrimental effects of overpronation should not be overlooked.
Surgical Treatment
Depending on the severity of your condition, your surgeon may recommend one or more treatment options. Ultimately, however, it's YOUR decision as to which makes the most sense to you. There are many resources available online and elsewhere for you to research the various options and make an informed decision.
Pronation is the inward movement of the foot as it rolls to distribute the force of impact of the ground as you run. The foot "rolls" inward about fifteen percent, comes in complete contact with the ground, and can support your body weight without any problem. Pronation is critical to proper shock absorption, and it helps you push off evenly from the front of the foot. Although pronation is a natural movement of the foot, the size of the arch can affect its ability to roll, causing either supination (underpronation) or overpronation. If you have a normal arch, you're likely a normal pronator, meaning you'll do best in a shoe that offers moderate pronation control. People with flat feet normally overpronate, so they do well in a motion-control shoe that controls pronation. High-arched people typically underpronate, so they do best in a neutral-cushioned shoe that encourages a more natural foot motion.
Causes
During our development, the muscles, ligaments, and other soft tissue structures that hold our bones together at the joints become looser than normal. When the bones are not held tightly in place, the joints are not aligned properly, and the foot gradually turns outward at the ankle, causing the inner ankle bone to appear more prominent. The foot moves in this direction because it is the path of least resistance. It is more difficult for the foot to move in the opposite direction (this is called supination). As we develop, the muscles and ligaments accommodate to this abnormal alignment. By the time growth is complete, the pronated foot is: abnormally flexible, flat, and its outer border appears raised so that as you step down you do not come down equally across the entire foot; instead, you come down mostly on the inner border of the foot. Normal aging will produce further laxity of our muscles that causes the pronation to become gradually worse.
Symptoms
Over-pronation is a condition where the arch flattens out which makes the feet roll inward while walking. This condition is also known as flat feet. It imposes extreme additional stresses on the plantar fascia, a fibrous band of tissue which connects the heel to the forefoot. Over-pronation makes walking a painful experience because of the additional strain on the calves, heel and/or back. Treatment for over-pronation involves the use of specially-made orthotics which offers arch support and medial rear foot posting as corrective measures.
Diagnosis
The best way to discover whether you have a normal gait, or if you overpronate, is to visit a specialty run shop, an exercise physiologist, a podiatrist or a physical therapist who specializes in working with athletes. A professional can analyze your gait, by watching you either walk or run, preferably on a treadmill. Some facilities can videotape your gait, then analyze the movement of your feet in slow-motion. Another (and less costly) way is to look at the bottom of an older pair of run shoes. Check the wear pattern. A person with a normal gait will generally see wear evenly across the heel and front of the shoe. A person who overpronates will likely see more wear on the OUTside of the heel and more wear on the INside of the forefoot (at the ball). A person who supinates will see wear all along the outer edges of the shoe. You can also learn about your gait by looking at your arches. Look at the shape your wet feet leave on a piece of paper or a flat walking surface.
Non Surgical Treatment
Overpronation is usually corrected with orthotics and/or strengthening exercises for the tibialis posterior. Massage treatment can relieve myofascial trigger points in the tibialis posterior, and other muscles, and address any resulting neuromuscular dysfunction in the leg or foot. Biomechanical correction of overpronation might require orthotics, neuromuscular reeducation, or gait retraining methods, as well. Stretching the gastrocnemius and soleus muscles will reduce hypertonicity in these muscles and also is essential for effective treatment. Because of impacts throughout the remainder of the body, the detrimental effects of overpronation should not be overlooked.
Surgical Treatment
Depending on the severity of your condition, your surgeon may recommend one or more treatment options. Ultimately, however, it's YOUR decision as to which makes the most sense to you. There are many resources available online and elsewhere for you to research the various options and make an informed decision.
Severs Disease The Facts
Overview
Heel pain in children and adolescence: is the most common osteochondrosis (disease that affects the bone growth). Osteochondrosis is seen only in children and teens whose bones are still growing of the foot. Sever's disease or Apophysitis is a common condition that afflicts children usually between the ages of 8 to 15 years old. Often this is confused with plantar fasciitis which is rare in children. This is a condition of inflammation of the heel's growth plates.
Causes
During the growth spurt of early puberty, the heel bone (also called the calcaneus) sometimes grows faster than the leg muscles and tendons. This can cause the muscles and tendons to become very tight and overstretched, making the heel less flexible and putting pressure on the growth plate. The Achilles tendon (also called the heel cord) is the strongest tendon that attaches to the growth plate in the heel. Over time, repeated stress (force or pressure) on the already tight Achilles tendon damages the growth plate, causing the swelling, tenderness, and pain of Sever's disease. Such stress commonly results from physical activities and sports that involve running and jumping, especially those that take place on hard surfaces, such as track, basketball, soccer, and gymnastics.
Symptoms
Sharp pain will be present in the affected heel (or both heels), especially while running or walking. Pain can be heightened following activity. The area will be tender to the touch and usually becomes inflamed or reddened. It may also be painful to press on the heel with a finger from the back or to squeeze the sides together; the latter is particularly common. You might notice stiffness in some of the surrounding muscles, making regular movements more difficult to achieve. This and the pain can manifest physically in abnormal practices like tiptoeing or limping. In some cases a lump can be detected on the back of the heel, though it may be so small as to defy detection.
Diagnosis
Sever?s disease can be diagnosed based on the symptoms your child has. Your child?s doctor will conduct a physical examination by squeezing different parts of your child?s foot to see if they cause any pain. An X-ray may be used to rule out other problems, such as a broken bone or fracture.
Non Surgical Treatment
Sever?s disease treatment should be based on eliminating pain and restoring normal foot and leg biomechanics. As with most soft tissue injuries the initial treatment is Rest, Ice, and Protect. In the early phase you?ll most likely be unable to walk pain-free. Our first aim is to provide you with some active rest from pain-provoking activities. "No Pain. No Gain." does not apply in Sever's disease. If it hurts your child is doing too much exercise. Your child should reduce or cease any activity that causes heel pain. Ice is a simple and effective modality to reduce your pain and swelling. Please apply for 20-30 minutes each 2 to 4 hours during the initial phase or when you notice that your injury is warm or hot. Most children can tolerate paracetamol as a pain reducing medication. Check with your doctor. To support and protect your heels, you may need to be wear shock absorbing heel cups or a soft orthotic. Kinesio foot taping may help to provide pain relief. Your physiotherapist will guide you and utilise a range of pain relieving techniques including joint mobilisations for stiff ankle or subtalar joints, massage or electrotherapy to assist you during this pain-full phase.
Exercise
The following exercises are commonly prescribed to patients with Severs disease. You should discuss the suitability of these exercises with your physiotherapist prior to beginning them. Generally, they should be performed 1 - 3 times daily and only provided they do not cause or increase symptoms. Your physiotherapist can advise when it is appropriate to begin the initial exercises and eventually progress to the intermediate, advanced and other exercises. As a general rule, addition of exercises or progression to more advanced exercises should take place provided there is no increase in symptoms. Calf Stretch with Towel. Begin this stretch in long sitting with your leg to be stretched in front of you. Your knee and back should be straight and a towel or rigid band placed around your foot as demonstrated. Using your foot, ankle and the towel, bring your toes towards your head as far as you can go without pain and provided you feel no more than a mild to moderate stretch in the back of your calf, Achilles tendon or leg. Hold for 5 seconds and repeat 10 times at a mild to moderate stretch provided the exercise is pain free. Calf Stretch with Towel. Begin this exercise with a resistance band around your foot and your foot and ankle held up towards your head. Slowly move your foot and ankle down against the resistance band as far as possible and comfortable without pain, tightening your calf muscle. Very slowly return back to the starting position. Repeat 10 - 20 times provided the exercise is pain free. Once you can perform 20 repetitions consistently without pain, the exercise can be progressed by gradually increasing the resistance of the band provided there is no increase in symptoms. Bridging. Begin this exercise lying on your back in the position demonstrated. Slowly lift your bottom pushing through your feet, until your knees, hips and shoulders are in a straight line. Tighten your bottom muscles (gluteals) as you do this. Hold for 2 seconds then slowly lower your bottom back down. Repeat 10 times provided the exercise is pain free.
Heel pain in children and adolescence: is the most common osteochondrosis (disease that affects the bone growth). Osteochondrosis is seen only in children and teens whose bones are still growing of the foot. Sever's disease or Apophysitis is a common condition that afflicts children usually between the ages of 8 to 15 years old. Often this is confused with plantar fasciitis which is rare in children. This is a condition of inflammation of the heel's growth plates.
Causes
During the growth spurt of early puberty, the heel bone (also called the calcaneus) sometimes grows faster than the leg muscles and tendons. This can cause the muscles and tendons to become very tight and overstretched, making the heel less flexible and putting pressure on the growth plate. The Achilles tendon (also called the heel cord) is the strongest tendon that attaches to the growth plate in the heel. Over time, repeated stress (force or pressure) on the already tight Achilles tendon damages the growth plate, causing the swelling, tenderness, and pain of Sever's disease. Such stress commonly results from physical activities and sports that involve running and jumping, especially those that take place on hard surfaces, such as track, basketball, soccer, and gymnastics.
Symptoms
Sharp pain will be present in the affected heel (or both heels), especially while running or walking. Pain can be heightened following activity. The area will be tender to the touch and usually becomes inflamed or reddened. It may also be painful to press on the heel with a finger from the back or to squeeze the sides together; the latter is particularly common. You might notice stiffness in some of the surrounding muscles, making regular movements more difficult to achieve. This and the pain can manifest physically in abnormal practices like tiptoeing or limping. In some cases a lump can be detected on the back of the heel, though it may be so small as to defy detection.
Diagnosis
Sever?s disease can be diagnosed based on the symptoms your child has. Your child?s doctor will conduct a physical examination by squeezing different parts of your child?s foot to see if they cause any pain. An X-ray may be used to rule out other problems, such as a broken bone or fracture.
Non Surgical Treatment
Sever?s disease treatment should be based on eliminating pain and restoring normal foot and leg biomechanics. As with most soft tissue injuries the initial treatment is Rest, Ice, and Protect. In the early phase you?ll most likely be unable to walk pain-free. Our first aim is to provide you with some active rest from pain-provoking activities. "No Pain. No Gain." does not apply in Sever's disease. If it hurts your child is doing too much exercise. Your child should reduce or cease any activity that causes heel pain. Ice is a simple and effective modality to reduce your pain and swelling. Please apply for 20-30 minutes each 2 to 4 hours during the initial phase or when you notice that your injury is warm or hot. Most children can tolerate paracetamol as a pain reducing medication. Check with your doctor. To support and protect your heels, you may need to be wear shock absorbing heel cups or a soft orthotic. Kinesio foot taping may help to provide pain relief. Your physiotherapist will guide you and utilise a range of pain relieving techniques including joint mobilisations for stiff ankle or subtalar joints, massage or electrotherapy to assist you during this pain-full phase.
Exercise
The following exercises are commonly prescribed to patients with Severs disease. You should discuss the suitability of these exercises with your physiotherapist prior to beginning them. Generally, they should be performed 1 - 3 times daily and only provided they do not cause or increase symptoms. Your physiotherapist can advise when it is appropriate to begin the initial exercises and eventually progress to the intermediate, advanced and other exercises. As a general rule, addition of exercises or progression to more advanced exercises should take place provided there is no increase in symptoms. Calf Stretch with Towel. Begin this stretch in long sitting with your leg to be stretched in front of you. Your knee and back should be straight and a towel or rigid band placed around your foot as demonstrated. Using your foot, ankle and the towel, bring your toes towards your head as far as you can go without pain and provided you feel no more than a mild to moderate stretch in the back of your calf, Achilles tendon or leg. Hold for 5 seconds and repeat 10 times at a mild to moderate stretch provided the exercise is pain free. Calf Stretch with Towel. Begin this exercise with a resistance band around your foot and your foot and ankle held up towards your head. Slowly move your foot and ankle down against the resistance band as far as possible and comfortable without pain, tightening your calf muscle. Very slowly return back to the starting position. Repeat 10 - 20 times provided the exercise is pain free. Once you can perform 20 repetitions consistently without pain, the exercise can be progressed by gradually increasing the resistance of the band provided there is no increase in symptoms. Bridging. Begin this exercise lying on your back in the position demonstrated. Slowly lift your bottom pushing through your feet, until your knees, hips and shoulders are in a straight line. Tighten your bottom muscles (gluteals) as you do this. Hold for 2 seconds then slowly lower your bottom back down. Repeat 10 times provided the exercise is pain free.
Flat Foot Symptoms In Adults
Overview
The posterior tibial tendon serves as one of the major supporting structures of the foot, helping it to function while walking. Posterior tibial tendon dysfunction (PTTD) is a condition caused by changes in the tendon, impairing its ability to support the arch. This results in flattening of the foot. PTTD is often called ?adult acquired flatfoot? because it is the most common type of flatfoot developed during adulthood. Although this condition typically occurs in only one foot, some people may develop it in both feet. PTTD is usually progressive, which means it will keep getting worse, especially if it isn?t treated early. 
Causes
Adult flatfoot typically occurs very gradually. If often develops in an obese person who already has somewhat flat feet. As the person ages, the tendons and ligaments that support the foot begin to lose their strength and elasticity.
Symptoms
Not everyone with adult flatfoot has problems with pain. Those who do usually experience it around the ankle or in the heel. The pain is usually worse with activity, like walking or standing for extended periods. Sometimes, if the condition develops from arthritis in the foot, bony spurs along the top and side of the foot develop and make wearing shoes more painful. Diabetic patients need to watch for swelling or large lumps in the feet, as they may not notice any pain. They are also at higher risk for developing significant deformities from their flatfoot.
Diagnosis
First, both feet should be examined with the patient standing and the entire lower extremity visible. The foot should be inspected from above as well as from behind the patient, as valgus angulation of the hindfoot is best appreciated when the foot is viewed from behind. Johnson described the so-called more-toes sign: with more advanced deformity and abduction of the forefoot, more of the lateral toes become visible when the foot is viewed from behind. The single-limb heel-rise test is an excellent determinant of the function of the posterior tibial tendon. The patient is asked to attempt to rise onto the ball of one foot while the other foot is suspended off the floor. Under normal circumstances, the posterior tibial muscle, which inverts and stabilizes the hindfoot, is activated as the patient begins to rise onto the forefoot. The gastrocnemius-soleus muscle group then elevates the calcaneus, and the heel-rise is accomplished. With dysfunction of the posterior tibial tendon, however, inversion of the heel is weak, and either the heel remains in valgus or the patient is unable to rise onto the forefoot. If the patient can do a single-limb heel-rise, the limb may be stressed further by asking the patient to perform this maneuver repetitively.
Non surgical Treatment
A patient who has acute tenosynovitis has pain and swelling along the medial aspect of the ankle. The patient is able to perform a single-limb heel-rise test but has pain when doing so. Inversion of the foot against resistance is painful but still strong. The patient should be managed with rest, the administration of appropriate anti-inflammatory medication, and immobilization. The injection of corticosteroids is not recommended. Immobilization with either a rigid below-the-knee cast or a removable cast or boot may be used to prevent overuse and subsequent rupture of the tendon. A removable stirrup-brace is not initially sufficient as it does not limit motion in the sagittal plane, a component of the pathological process. The patient should be permitted to walk while wearing the cast or boot during the six to eight-week period of immobilization. At the end of that time, a decision must be made regarding the need for additional treatment. If there has been marked improvement, the patient may begin wearing a stiff-soled shoe with a medial heel-and-sole wedge to invert the hindfoot. If there has been only mild or moderate improvement, a longer period in the cast or boot may be tried. 
Surgical Treatment
For patients with a more severe deformity, or significant symptoms that do not respond to conservative treatment, surgery may be necessary. There are several procedures available depending on the nature of your condition. Ligament and muscle lengthening, removal of inflamed tendon lining, transferring of a nearby tendon to re-establish an arch, and bone realignment and fusion are examples of surgical options to help with a painful flatfoot condition. Surgery can be avoided when symptoms are addressed early. If you are feeling ankle pain or notice any warmth, redness or swelling in your foot, contact us immediately. We can create a tailored treatment plan to resolve your symptoms and prevent future problems.
Do You Really Understand Heel Soreness?
Overview

Does your heel feel painful when you get up from bed every morning, or when you get up after sitting down for a long period of time? If you often experience this sort of pain, known as first step pain, you could be suffering from plantar fasciitis (pronounced fash-ee-eye-tus), an inflammation of the plantar fascia, or the band of muscle under the foot. Plantar fasciitis is the most common cause of Heel Pain.
Causes
Heel pain sometimes results from excessive pronation. Pronation is the normal flexible motion and flattening of the arch of the foot that allows it to adapt to ground surfaces and absorb shock in the normal walking pattern. As you walk, the heel contacts the ground first; the weight shifts first to the outside of the foot, then moves toward the big toe. The arch rises, the foot generally rolls upward and outward, becoming rigid and stable in order to lift the body and move it forward. Excessive pronation-excessive inward motion-can create an abnormal amount of stretching and pulling on the ligaments and tendons attaching to the bottom back of the heel bone. Excessive pronation may also contribute to injury to the hip, knee, and lower back.
Symptoms
The most common complaint is pain and stiffness in the bottom of the heel. Heel pain may be sharp or dull, and it may develop slowly over time or suddenly after intense activity. The pain is typically worse in the morning, when taking your first steps of the day. After standing or sitting for a while. When climbing stairs.
Diagnosis
After you have described your foot symptoms, your doctor will want to know more details about your pain, your medical history and lifestyle, including. Whether your pain is worse at specific times of the day or after specific activities. Any recent injury to the area. Your medical and orthopedic history, especially any history of diabetes, arthritis or injury to your foot or leg. Your age and occupation. Your recreational activities, including sports and exercise programs. The type of shoes you usually wear, how well they fit, and how frequently you buy a new pair. Your doctor will examine you, including. An evaluation of your gait. While you are barefoot, your doctor will ask you to stand still and to walk in order to evaluate how your foot moves as you walk. An examination of your feet. Your doctor may compare your feet for any differences between them. Then your doctor may examine your painful foot for signs of tenderness, swelling, discoloration, muscle weakness and decreased range of motion. A neurological examination. The nerves and muscles may be evaluated by checking strength, sensation and reflexes. In addition to examining you, your health care professional may want to examine your shoes. Signs of excessive wear in certain parts of a shoe can provide valuable clues to problems in the way you walk and poor bone alignment. Depending on the results of your physical examination, you may need foot X-rays or other diagnostic tests.
Non Surgical Treatment
Treatment for heel pain usually involves using a combination of techniques, such as stretches and painkillers, to relieve pain and speed up recovery. Most cases of heel pain get better within 12 months. Surgery may be recommended as a last resort if your symptoms don't improve after this time. Only 1 in 20 people with heel pain will need surgery. Whenever possible, rest the affected foot by not walking long distances and standing for long periods. However, you should regularly stretch your feet and calves using exercises such as those described. Non-steroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, can be used to help relieve pain. Some people also find applying an ice pack to the affected heel for 5-10 minutes can help relieve pain and inflammation. However, do not apply an ice pack directly to your skin. Instead, wrap it in a towel. If you do not have an ice pack, you can use a packet of frozen vegetables. Exercises designed to stretch both your calf muscles and your plantar fascia (the band of tissue that runs under the sole of your foot) should help relieve pain and improve flexibility in the affected foot. A number of stretching exercises are described below. It's usually recommended that you do the exercises on both legs, even if only one of your heels is affected by pain. This will improve your balance and stability, and help relieve heel pain. Keep a long towel beside your bed. Before you get out of bed in the morning, loop the towel around your foot and use it to pull your toes towards your body, while keeping your knee straight. Repeat three times on each foot. Place both hands on a wall at shoulder height, with one of your feet in front of the other. The front foot should be about 30cm (12 inches) away from the wall. With your front knee bent and your back leg straight, lean towards the wall until you feel a tightening in the calf muscles of your back leg. Then relax. Repeat this exercise 10 times before switching legs and repeating the cycle. You should practise wall stretches twice a day. Stand on a step of your stairs facing upstairs, using your banister for support. Your feet should be slightly apart, with your heels hanging off the back of the step. Lower your heels until you feel a tightening in your calves. Hold this position for about 40 seconds, before raising your heels back to the starting position. Repeat this procedure six times, at least twice a day. Sit on a chair, with your knees bent at right angles. Turn your feet sideways so your heels are touching and your toes are pointing in opposite directions. Lift the toes of the affected foot upwards, while keeping the heel firmly on the floor. You should feel your calf muscles and Achilles tendon (the band of tissue that connects your heel bone to your calf muscle) tighten. Hold this position for several seconds and then relax. Repeat this procedure 10 times, five to six times a day. While seated, roll the arch of your foot (the curved bottom part of the foot between your toes and heel) over a round object, such as a rolling pin, tennis ball or drinks can. Some people find that using a chilled can from their fridge has the added benefit of helping to relieve pain. Move your foot and ankle in all directions over the object for several minutes. Repeat the exercise twice a day. Your GP or podiatrist may advise you to change your footwear. You should avoid wearing flat-soled shoes, because they will not provide your heel with support and could make your heel pain worse. Ideally, you should wear shoes that cushion your heels and provide a good level of support to the arches of your feet. For women wearing high heels, and for men wearing heeled boots or brogues, can provide short- to medium-term pain relief, as they help reduce pressure on the heels. However, these types of shoes may not be suitable in the long term, because they can lead to further episodes of heel pain. Your GP or podiatrist can advise on footwear. Orthoses are insoles that fit inside your shoe to support your foot and help your heel recover. You can buy orthoses off-the-shelf from sports shops and larger pharmacies. Alternatively, your podiatrist should be able to recommend a supplier. If your pain does not respond to treatment and keeps recurring, or if you have an abnormal foot shape or structure, custom-made orthoses are available. These are specifically made to fit the shape of your feet. However, there is currently no evidence to suggest that custom-made orthoses are more effective than those bought off-the-shelf. An alternative to using orthoses is to have your heel strapped with sports strapping (zinc oxide) tape, which helps relieve pressure on your heel. Your GP or podiatrist can teach you how to apply the tape yourself. In some cases, night splints can also be useful. Most people sleep with their toes pointing down, which means tissue inside the heel is squeezed together. Night splints, which look like boots, are designed to keep your toes and feet pointing up while you are asleep. This will stretch both your Achilles tendon and your plantar fascia, which should help speed up your recovery time. Night splints are usually only available from specialist shops and online retailers. Again, your podiatrist should be able to recommend a supplier. If treatment hasn't helped relieve your painful symptoms, your GP may recommend corticosteroid injections. Corticosteroids are a type of medication that have a powerful anti-inflammatory effect. They have to be used sparingly because overuse can cause serious side effects, such as weight gain and high blood pressure (hypertension). As a result, it is usually recommended that no more than three corticosteroid injections are given within a year in any part of the body. Before having a corticosteroid injection, a local anaesthetic may be used to numb your foot so you don't feel any pain.
Surgical Treatment
If treatment hasn't worked and you still have painful symptoms after a year, your GP may refer you to either an orthopaedic surgeon, a surgeon who specialises in surgery that involves bones, muscles and joints or a podiatric surgeon, a podiatrist who specialises in foot surgery. Surgery is sometimes recommended for professional athletes and other sportspeople whose heel pain is adversely affecting their career. Plantar release surgery is the most widely used type of surgery for heel pain. The surgeon will cut the fascia to release it from your heel bone and reduce the tension in your plantar fascia. This should reduce any inflammation and relieve your painful symptoms. Surgery can be performed either as open surgery, where the section of the plantar fascia is released by making a cut into your heel or endoscopic or minimal incision surgery - where a smaller incision is made and special instruments are inserted through the incision to gain access to the plantar fascia. Endoscopic or minimal incision surgery has a quicker recovery time, so you will be able to walk normally much sooner (almost immediately), compared with two to three weeks for open surgery. A disadvantage of endoscopic surgery is that it requires both a specially trained surgical team and specialised equipment, so you may have to wait longer for treatment than if you were to choose open surgery. Endoscopic surgery also carries a higher risk of damaging nearby nerves, which could result in symptoms such as numbness, tingling or some loss of movement in your foot. As with all surgery, plantar release carries the risk of causing complications such as infection, nerve damage and a worsening of your symptoms after surgery (although this is rare). You should discuss the advantages and disadvantages of both techniques with your surgical team.
Prevention

A variety of steps can be taken to avoid heel pain and accompanying afflictions. Wear shoes that fit well-front, back, and sides-and have shock-absorbent soles, rigid shanks, and supportive heel counters. Wear the proper shoes for each activity. Do not wear shoes with excessive wear on heels or soles. Prepare properly before exercising. Warm up and do stretching exercises before and after running. Pace yourself when you participate in athletic activities. Don't underestimate your body's need for rest and good nutrition. If obese, lose weight.
Does your heel feel painful when you get up from bed every morning, or when you get up after sitting down for a long period of time? If you often experience this sort of pain, known as first step pain, you could be suffering from plantar fasciitis (pronounced fash-ee-eye-tus), an inflammation of the plantar fascia, or the band of muscle under the foot. Plantar fasciitis is the most common cause of Heel Pain.
Causes
Heel pain sometimes results from excessive pronation. Pronation is the normal flexible motion and flattening of the arch of the foot that allows it to adapt to ground surfaces and absorb shock in the normal walking pattern. As you walk, the heel contacts the ground first; the weight shifts first to the outside of the foot, then moves toward the big toe. The arch rises, the foot generally rolls upward and outward, becoming rigid and stable in order to lift the body and move it forward. Excessive pronation-excessive inward motion-can create an abnormal amount of stretching and pulling on the ligaments and tendons attaching to the bottom back of the heel bone. Excessive pronation may also contribute to injury to the hip, knee, and lower back.
Symptoms
The most common complaint is pain and stiffness in the bottom of the heel. Heel pain may be sharp or dull, and it may develop slowly over time or suddenly after intense activity. The pain is typically worse in the morning, when taking your first steps of the day. After standing or sitting for a while. When climbing stairs.
Diagnosis
After you have described your foot symptoms, your doctor will want to know more details about your pain, your medical history and lifestyle, including. Whether your pain is worse at specific times of the day or after specific activities. Any recent injury to the area. Your medical and orthopedic history, especially any history of diabetes, arthritis or injury to your foot or leg. Your age and occupation. Your recreational activities, including sports and exercise programs. The type of shoes you usually wear, how well they fit, and how frequently you buy a new pair. Your doctor will examine you, including. An evaluation of your gait. While you are barefoot, your doctor will ask you to stand still and to walk in order to evaluate how your foot moves as you walk. An examination of your feet. Your doctor may compare your feet for any differences between them. Then your doctor may examine your painful foot for signs of tenderness, swelling, discoloration, muscle weakness and decreased range of motion. A neurological examination. The nerves and muscles may be evaluated by checking strength, sensation and reflexes. In addition to examining you, your health care professional may want to examine your shoes. Signs of excessive wear in certain parts of a shoe can provide valuable clues to problems in the way you walk and poor bone alignment. Depending on the results of your physical examination, you may need foot X-rays or other diagnostic tests.
Non Surgical Treatment
Treatment for heel pain usually involves using a combination of techniques, such as stretches and painkillers, to relieve pain and speed up recovery. Most cases of heel pain get better within 12 months. Surgery may be recommended as a last resort if your symptoms don't improve after this time. Only 1 in 20 people with heel pain will need surgery. Whenever possible, rest the affected foot by not walking long distances and standing for long periods. However, you should regularly stretch your feet and calves using exercises such as those described. Non-steroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, can be used to help relieve pain. Some people also find applying an ice pack to the affected heel for 5-10 minutes can help relieve pain and inflammation. However, do not apply an ice pack directly to your skin. Instead, wrap it in a towel. If you do not have an ice pack, you can use a packet of frozen vegetables. Exercises designed to stretch both your calf muscles and your plantar fascia (the band of tissue that runs under the sole of your foot) should help relieve pain and improve flexibility in the affected foot. A number of stretching exercises are described below. It's usually recommended that you do the exercises on both legs, even if only one of your heels is affected by pain. This will improve your balance and stability, and help relieve heel pain. Keep a long towel beside your bed. Before you get out of bed in the morning, loop the towel around your foot and use it to pull your toes towards your body, while keeping your knee straight. Repeat three times on each foot. Place both hands on a wall at shoulder height, with one of your feet in front of the other. The front foot should be about 30cm (12 inches) away from the wall. With your front knee bent and your back leg straight, lean towards the wall until you feel a tightening in the calf muscles of your back leg. Then relax. Repeat this exercise 10 times before switching legs and repeating the cycle. You should practise wall stretches twice a day. Stand on a step of your stairs facing upstairs, using your banister for support. Your feet should be slightly apart, with your heels hanging off the back of the step. Lower your heels until you feel a tightening in your calves. Hold this position for about 40 seconds, before raising your heels back to the starting position. Repeat this procedure six times, at least twice a day. Sit on a chair, with your knees bent at right angles. Turn your feet sideways so your heels are touching and your toes are pointing in opposite directions. Lift the toes of the affected foot upwards, while keeping the heel firmly on the floor. You should feel your calf muscles and Achilles tendon (the band of tissue that connects your heel bone to your calf muscle) tighten. Hold this position for several seconds and then relax. Repeat this procedure 10 times, five to six times a day. While seated, roll the arch of your foot (the curved bottom part of the foot between your toes and heel) over a round object, such as a rolling pin, tennis ball or drinks can. Some people find that using a chilled can from their fridge has the added benefit of helping to relieve pain. Move your foot and ankle in all directions over the object for several minutes. Repeat the exercise twice a day. Your GP or podiatrist may advise you to change your footwear. You should avoid wearing flat-soled shoes, because they will not provide your heel with support and could make your heel pain worse. Ideally, you should wear shoes that cushion your heels and provide a good level of support to the arches of your feet. For women wearing high heels, and for men wearing heeled boots or brogues, can provide short- to medium-term pain relief, as they help reduce pressure on the heels. However, these types of shoes may not be suitable in the long term, because they can lead to further episodes of heel pain. Your GP or podiatrist can advise on footwear. Orthoses are insoles that fit inside your shoe to support your foot and help your heel recover. You can buy orthoses off-the-shelf from sports shops and larger pharmacies. Alternatively, your podiatrist should be able to recommend a supplier. If your pain does not respond to treatment and keeps recurring, or if you have an abnormal foot shape or structure, custom-made orthoses are available. These are specifically made to fit the shape of your feet. However, there is currently no evidence to suggest that custom-made orthoses are more effective than those bought off-the-shelf. An alternative to using orthoses is to have your heel strapped with sports strapping (zinc oxide) tape, which helps relieve pressure on your heel. Your GP or podiatrist can teach you how to apply the tape yourself. In some cases, night splints can also be useful. Most people sleep with their toes pointing down, which means tissue inside the heel is squeezed together. Night splints, which look like boots, are designed to keep your toes and feet pointing up while you are asleep. This will stretch both your Achilles tendon and your plantar fascia, which should help speed up your recovery time. Night splints are usually only available from specialist shops and online retailers. Again, your podiatrist should be able to recommend a supplier. If treatment hasn't helped relieve your painful symptoms, your GP may recommend corticosteroid injections. Corticosteroids are a type of medication that have a powerful anti-inflammatory effect. They have to be used sparingly because overuse can cause serious side effects, such as weight gain and high blood pressure (hypertension). As a result, it is usually recommended that no more than three corticosteroid injections are given within a year in any part of the body. Before having a corticosteroid injection, a local anaesthetic may be used to numb your foot so you don't feel any pain.
Surgical Treatment
If treatment hasn't worked and you still have painful symptoms after a year, your GP may refer you to either an orthopaedic surgeon, a surgeon who specialises in surgery that involves bones, muscles and joints or a podiatric surgeon, a podiatrist who specialises in foot surgery. Surgery is sometimes recommended for professional athletes and other sportspeople whose heel pain is adversely affecting their career. Plantar release surgery is the most widely used type of surgery for heel pain. The surgeon will cut the fascia to release it from your heel bone and reduce the tension in your plantar fascia. This should reduce any inflammation and relieve your painful symptoms. Surgery can be performed either as open surgery, where the section of the plantar fascia is released by making a cut into your heel or endoscopic or minimal incision surgery - where a smaller incision is made and special instruments are inserted through the incision to gain access to the plantar fascia. Endoscopic or minimal incision surgery has a quicker recovery time, so you will be able to walk normally much sooner (almost immediately), compared with two to three weeks for open surgery. A disadvantage of endoscopic surgery is that it requires both a specially trained surgical team and specialised equipment, so you may have to wait longer for treatment than if you were to choose open surgery. Endoscopic surgery also carries a higher risk of damaging nearby nerves, which could result in symptoms such as numbness, tingling or some loss of movement in your foot. As with all surgery, plantar release carries the risk of causing complications such as infection, nerve damage and a worsening of your symptoms after surgery (although this is rare). You should discuss the advantages and disadvantages of both techniques with your surgical team.
Prevention
A variety of steps can be taken to avoid heel pain and accompanying afflictions. Wear shoes that fit well-front, back, and sides-and have shock-absorbent soles, rigid shanks, and supportive heel counters. Wear the proper shoes for each activity. Do not wear shoes with excessive wear on heels or soles. Prepare properly before exercising. Warm up and do stretching exercises before and after running. Pace yourself when you participate in athletic activities. Don't underestimate your body's need for rest and good nutrition. If obese, lose weight.
What Can Cause Tendonitis Discomfort Of The Achilles ?
Overview
 Do you experience dull pain near the back of your heel or in the back of your leg after your regular run or after playing your favourite sport? When you ramp up your exercise is the pain more severe or prolonged? If so, you may have Achilles tendinitis. The Achilles tendon is the thick, strong, springy band of tissue that connects the muscles from the middle of your calf to your heel bone. You use your Achilles tendon when you walk, run or jump. Achilles tendinitis occurs when the Achilles tendon is repeatedly strained. The Achilles tendon becomes less flexible, weaker and more prone to injury as we age. Middle-aged weekend warriors and runners who suddenly intensify their training often suffer from Achilles tendinitis.
Do you experience dull pain near the back of your heel or in the back of your leg after your regular run or after playing your favourite sport? When you ramp up your exercise is the pain more severe or prolonged? If so, you may have Achilles tendinitis. The Achilles tendon is the thick, strong, springy band of tissue that connects the muscles from the middle of your calf to your heel bone. You use your Achilles tendon when you walk, run or jump. Achilles tendinitis occurs when the Achilles tendon is repeatedly strained. The Achilles tendon becomes less flexible, weaker and more prone to injury as we age. Middle-aged weekend warriors and runners who suddenly intensify their training often suffer from Achilles tendinitis.
Causes
Achilles tendinitis can be caused by any activity that puts stress on your Achilles tendon. Tendinitis can develop if you run or jump more than usual or exercise on a hard surface. Tendinitis can be caused by shoes that do not fit or support your foot and ankle. Tight tendons and muscles, You may have tight hamstring and calf muscles in your upper and lower leg. Your tendons also become stiffer and easier to injure as you get older. Arthritis, Bony growths caused by arthritis can irritate the Achilles tendon, especially around your heel.
Symptoms
The primary symptom of Achilles tendon inflammation is pain in the back of the heel, which initially increases when exercise is begun and often lessens as exercise continues. A complete tear of the Achilles tendon typically occurs with a sudden forceful change in direction when running or playing tennis and is often accompanied by a sensation of having been struck in the back of the ankle and calf with an object such as a baseball bat.
Diagnosis
During an examination of the foot and ankle, you doctor will look for the following signs, Achilles tendon swelling or thickening. Bone spurs appearing at the lower part of the tendon at the back of the hell. Pain at the middle or lower area of the Achilles tendon. Limited range of motion of the foot and ankle, and a decreased ability to flex the foot. Your doctor may perform imaging tests, such as X-rays and MRI scans, to make a diagnosis of Achilles tendinitis. X-rays show images of the bones and can help the physician to determine if the Achilles tendon has become hardened, which indicated insertional Achilles tendinitis. MRI scans may not be necessary, but they are important guides if you are recommended to have surgical treatment. An MRI can show the severity of the damage and determine what kind of procedure would be best to address the condition.
Nonsurgical Treatment
Treatment options might include anti-inflammatory medication such as ibuprofen which might help with acute achilles inflammation and pain but has not been proven to be beneficial long term and may even inhibit healing. If the injury is severe then a plaster cast might be applied to immobilize the tendon. Use of electrotherapy such as ultrasound treatment, laser therapy and extracorporeal shock wave therapy (ESWT) may be beneficial in reducing pain and encouraging healing. Applying sports massage techniques can mobilze the tissues or the tendon itself and help stretch the calf muscles. Some might give a steroid injection however an injection directly into the tendon is not recommended. Some specialists believe this can increase the risk of a total rupture of the tendon in future. One of the most effective forms of treatment for achilles tendonitis is a full rehabilitation program consisting of eccentric strengthening exercises. There is now considerable evidence suggesting the effectiveness of slow eccentric rehabilitation exercises for curing achilles tendon pain.

Surgical Treatment
Around 1 in 4 people who have persisting pain due to Achilles tendinopathy has surgery to treat the condition. Most people have a good result from surgery and their pain is relieved. Surgery involves either of the following, removing nodules or adhesions (parts of the fibres of the tendon that have stuck together) that have developed within the damaged tendon. Making a lengthways cut in the tendon to help to stimulate and encourage tendon healing. Complications from surgery are not common but, if they do occur, can include problems with wound healing.
Prevention
To prevent Achilles tendonitis or tendonosis from recurring after surgical or non-surgical treatment, the foot and ankle surgeon may recommend strengthening and stretching of the calf muscles through daily exercises. Wearing proper shoes for the foot type and activity is also important in preventing recurrence of the condition.
Do you experience dull pain near the back of your heel or in the back of your leg after your regular run or after playing your favourite sport? When you ramp up your exercise is the pain more severe or prolonged? If so, you may have Achilles tendinitis. The Achilles tendon is the thick, strong, springy band of tissue that connects the muscles from the middle of your calf to your heel bone. You use your Achilles tendon when you walk, run or jump. Achilles tendinitis occurs when the Achilles tendon is repeatedly strained. The Achilles tendon becomes less flexible, weaker and more prone to injury as we age. Middle-aged weekend warriors and runners who suddenly intensify their training often suffer from Achilles tendinitis.
Causes
Achilles tendinitis can be caused by any activity that puts stress on your Achilles tendon. Tendinitis can develop if you run or jump more than usual or exercise on a hard surface. Tendinitis can be caused by shoes that do not fit or support your foot and ankle. Tight tendons and muscles, You may have tight hamstring and calf muscles in your upper and lower leg. Your tendons also become stiffer and easier to injure as you get older. Arthritis, Bony growths caused by arthritis can irritate the Achilles tendon, especially around your heel.
Symptoms
The primary symptom of Achilles tendon inflammation is pain in the back of the heel, which initially increases when exercise is begun and often lessens as exercise continues. A complete tear of the Achilles tendon typically occurs with a sudden forceful change in direction when running or playing tennis and is often accompanied by a sensation of having been struck in the back of the ankle and calf with an object such as a baseball bat.
Diagnosis
During an examination of the foot and ankle, you doctor will look for the following signs, Achilles tendon swelling or thickening. Bone spurs appearing at the lower part of the tendon at the back of the hell. Pain at the middle or lower area of the Achilles tendon. Limited range of motion of the foot and ankle, and a decreased ability to flex the foot. Your doctor may perform imaging tests, such as X-rays and MRI scans, to make a diagnosis of Achilles tendinitis. X-rays show images of the bones and can help the physician to determine if the Achilles tendon has become hardened, which indicated insertional Achilles tendinitis. MRI scans may not be necessary, but they are important guides if you are recommended to have surgical treatment. An MRI can show the severity of the damage and determine what kind of procedure would be best to address the condition.
Nonsurgical Treatment
Treatment options might include anti-inflammatory medication such as ibuprofen which might help with acute achilles inflammation and pain but has not been proven to be beneficial long term and may even inhibit healing. If the injury is severe then a plaster cast might be applied to immobilize the tendon. Use of electrotherapy such as ultrasound treatment, laser therapy and extracorporeal shock wave therapy (ESWT) may be beneficial in reducing pain and encouraging healing. Applying sports massage techniques can mobilze the tissues or the tendon itself and help stretch the calf muscles. Some might give a steroid injection however an injection directly into the tendon is not recommended. Some specialists believe this can increase the risk of a total rupture of the tendon in future. One of the most effective forms of treatment for achilles tendonitis is a full rehabilitation program consisting of eccentric strengthening exercises. There is now considerable evidence suggesting the effectiveness of slow eccentric rehabilitation exercises for curing achilles tendon pain.
Surgical Treatment
Around 1 in 4 people who have persisting pain due to Achilles tendinopathy has surgery to treat the condition. Most people have a good result from surgery and their pain is relieved. Surgery involves either of the following, removing nodules or adhesions (parts of the fibres of the tendon that have stuck together) that have developed within the damaged tendon. Making a lengthways cut in the tendon to help to stimulate and encourage tendon healing. Complications from surgery are not common but, if they do occur, can include problems with wound healing.
Prevention
To prevent Achilles tendonitis or tendonosis from recurring after surgical or non-surgical treatment, the foot and ankle surgeon may recommend strengthening and stretching of the calf muscles through daily exercises. Wearing proper shoes for the foot type and activity is also important in preventing recurrence of the condition.
What Causes Pain Of The Heel
Overview
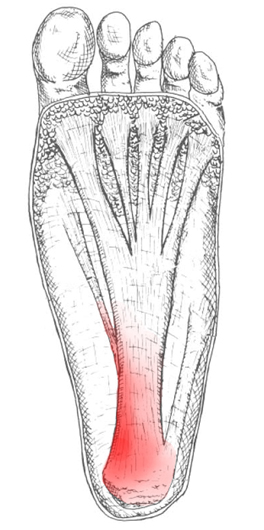
Plantar fasciitis is an inflammation of the structures (of the plantar fascia) on the sole of the foot. The inflammation is caused by excess pressure on the structures on the sole of the foot. The plantar fascia becomes inflamed and tiny rips can occur where it attaches into the inside of the heel bone. It tends to be most painful first thing in the morning, or when standing up after sitting for a while. The area becomes inflamed and swollen, and it is the increase in fluid to the area that accumulates when weight is taken off the area, that then causes the pain on standing. Plantar Fasciitis usually starts gradually with pain on standing after rest. Pain is usually located under the heel or to the inside of the heel. Pain is usually at its worst on standing first thing in the morning. The pain will begin to ease once you get moving. Pain in the early stages tends to occur after activity rather than during activity. As plantar fasciitis continues the pain can become more constant and can then start to affect the way you walk.
Causes
Plantar fasciitis is the most common injury of the plantar fascia and is the most common cause of heel pain. Approximately 10% of people have plantar fasciitis at some point during their lifetime. It is commonly associated with long periods of standing and is much more prevalent in individuals with excessive inward rolling of the foot, which is seen with flat feet. Among non-athletic populations, plantar fasciitis is associated with obesity and lack of physical exercise.
Symptoms
The most common symptoms of plantar fasciitis include pain on the bottom of the foot near the heel, pain with the first few steps after getting out of bed in the morning, or after a long period of rest, such as after a long car ride. The pain subsides after a few minutes of walking. Greater pain after (not during) exercise or activity.
Diagnosis
Physical examination is the best way to determine if you have plantar fasciitis. Your doctor examines the affected area to determine if plantar fasciitis is the cause of your pain. The doctor may also examine you while you are sitting, standing, and walking. It is important to discuss your daily routine with your doctor. An occupation in which you stand for long periods of time may cause plantar fasciitis. An X-ray may reveal a heel spur. The actual heel spur is not painful. The presence of a heel spur suggests that the plantar fascia has been pulled and stretched excessively for a long period of time, sometimes months or years. If you have plantar fasciitis, you may or may not have a heel spur. Even if your plantar fasciitis becomes less bothersome, the heel spur will remain.
Non Surgical Treatment
In general, we start by correcting training errors. This usually requires relative rest, the use of ice after activities, and an evaluation of the patient's shoes and activities. Next, we try correction of biomechanical factors with a stretching and strengthening program. If the patient still has no improvement, we consider night splints and orthotics. Finally, all other treatment options are considered. Non-steroidal anti-inflammatory medications are considered throughout the treatment course, although we explain to the patient that this medicine is being used primarily for pain control and not to treat the underlying problem.

Surgical Treatment
Surgery is rarely needed in the treatment of plantar fasciitis. The vast majority of patients diagnosed with plantar fasciitis will recover given ample time. With some basic treatment steps, well over 90% of patients will achieve full recovery from symptoms of plantar fasciitis within one year of the onset of treatment. Simple treatments include anti-inflammatory medication, shoe inserts, and stretching exercises. In patients where a good effort with these treatments fails to provide adequate relief, some more aggressive treatments may be attempted. These include cortisone injections or extracorporeal shock wave treatments.
Stretching Exercises
Stretching your plantar fasciitis is something you can do at home to relieve pain and speed healing. Ice massage performed three to four times per day in 15 to 20 minute intervals is also something you can do to reduce inflammation and pain. Placing arch supports in your shoes absorbs shock and takes pressure off the plantar fascia.